
More Information
Submitted: 21 February 2020 | Approved: 27 February 2020 | Published: 28 February 2020
How to cite this article: Munir S, Riaz S. Type 2 diabetes and cancer. Ann Clin Endocrinol Metabol. 2020; 4: 001-006.
DOI: 10.29328/journal.acem.1001012
ORCiD: orcid.org/0000-0001-8836-0710
Copyright License: © 2020 Munir S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Diabetes; Cancer mortality; Risk; Hyperinsulinemia; Metformin

Type 2 diabetes and cancer
Snobia Munir1* and Samreen Riaz2
1Research Scholar, Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore, Pakistan
2Assistant Professor, Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore, Pakistan
*Address for Correspondence: Snobia Munir, Research Scholar, Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore, Pakistan, Tel: 03158269694; Email: [email protected]
Diabetes mellitus increases the possibility of different cancers. Scientists have substantiated the link of diabetes with increased prevalence, augmented progression and improved cancer aggression. Research has strengthened link of diabetes with the colorectal cancer risk among various cancers. Diagnosis and treatment have made some progress in recent years, but Colorectal is major issue for the health of people even today. In order to reduce cancer mortality, there is importance of prophylaxis, evaluation and proper treatment. Factors distressing cancer prognosis is required by policy-making system for beneficial approaches of cancer patients and improvement of disease. Eventually diabetes- specific strategies for different cancers are explored.
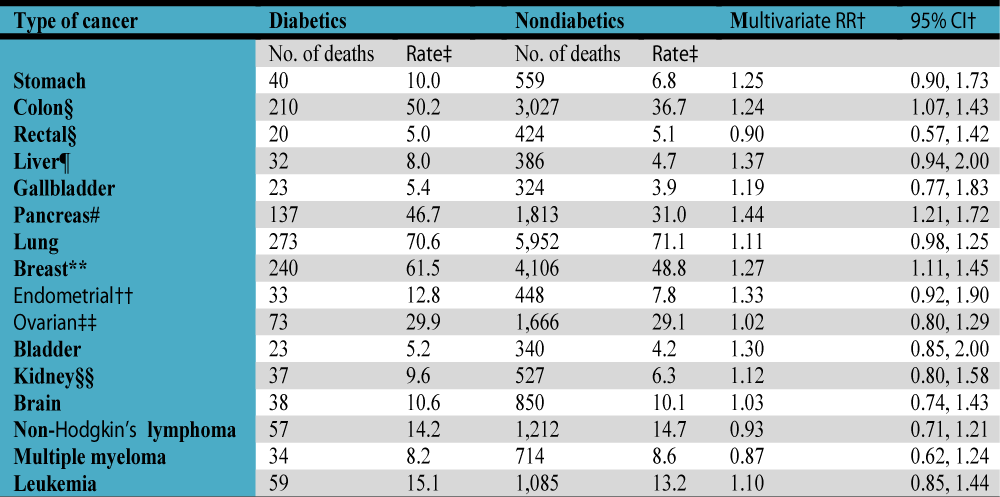
Type 2 diabetes can enhance risk of a varied range of tumors, for instance pancreas, liver, early gastric, ovarian, prostate, breast and colorectal cancer (Table 1). It is among communal prolonged diseases of the world affecting every sector of society comprising of females, young people and grown person. Diabetic women are more likely to develop an increased colorectal cancer incidence and mortality [1]. In most, but not all studies, diabetes was related to a greater chances of colorectal cancer. There have been non-conclusive findings in the colorectum on sex and subsite (Table 2). Data from a number of independent studies on interrelation of diabetes with colorectal cancer incidence and morbidity to resolve these inconsistencies has been conducted. The findings strongly support the link of diabetes with greater risk in population for colorectal cancer [2]. People with diabetes have about 30 percent higher relative menace of cancer than non-diabetic people [3]. The results in epidemiological observational studies were constant in Europe and United States. In both men and women and in all colorectal subsites, the relationship was witnessed.
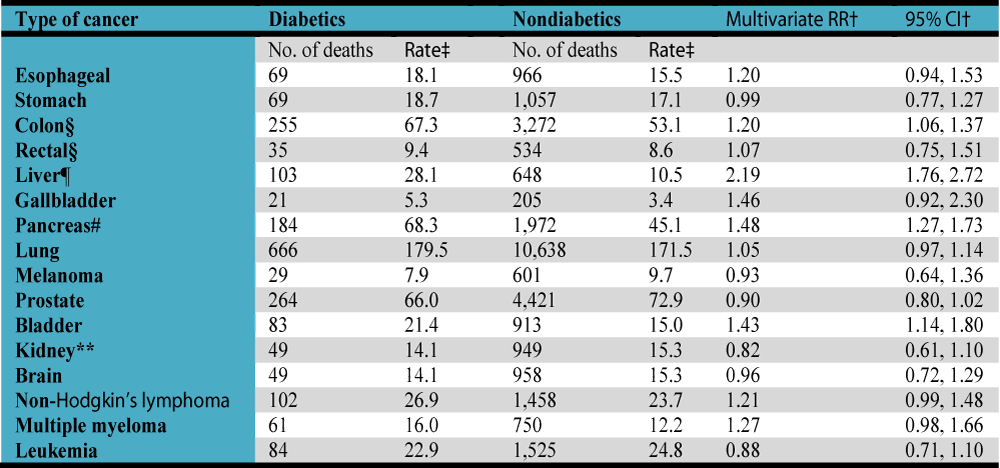
Table 1: Relation between diabetes and fatal cancers in men and women, American Cancer Society Cancer Prevention. *All analyses were adjusted for a core group of covariates (age, race, years of education, body mass index, cigarette smoking history, alcohol consumption, total red meat consumption, consumption of citrus fruits and juices, consumption of vegetables, physical activity). Except for melanoma, non-Hodgkin’s lymphoma, and multiple myeloma, analyses for each type of cancer were also adjusted for a family history of that cancer in a first-degree relative. †RR, relative risk; CI, confidence interval. ‡Mortality rate per 100,000 age standardized to the Cancer Prevention Study II male population. §Also adjusted for polyps, aspirin use, and consumption of whole grains. ¶also adjusted for hepatitis and cirrhosis. #also adjusted for history of gallstones. **also adjusted for hypertension.
*All analyses were adjusted for a core group of covariates (age, race, years of education, body mass index, cigarette smoking history, alcohol consumption, total red meat consumption, consumption of citrus fruits and juices, consumption of vegetables, physical activity, use of replacement estrogens). Except for gallbladder cancer, lung cancer, non-Hodgkin’s lymphoma, and multiple myeloma, analyses for each type of cancer were also adjusted for a family history of that cancer in a first-degree relative. †RR, relative risk; CI, confidence interval. ‡Mortality rate per 100,000 age standardized to the Cancer Prevention Study II female population. §also adjusted for polyps, aspirin use, and consumption of whole grains. ¶also adjusted for hepatitis and cirrhosis. #also adjusted for history of gallstones. **Also adjusted for parity, age at menarche, age at first live birth, and menopausal status. ††Excludes women who have had a hysterectomy. Also adjusted for parity, age at menarche, age at first livebirth, menopausal status, and oral contraceptive use. ‡‡Excludes women who have had a hysterectomy or oophorectomy. Also adjusted for parity, age at menarche, age at first livebirth, menopausal status, and oral contraceptive use. §§Also adjusted for hypertension.
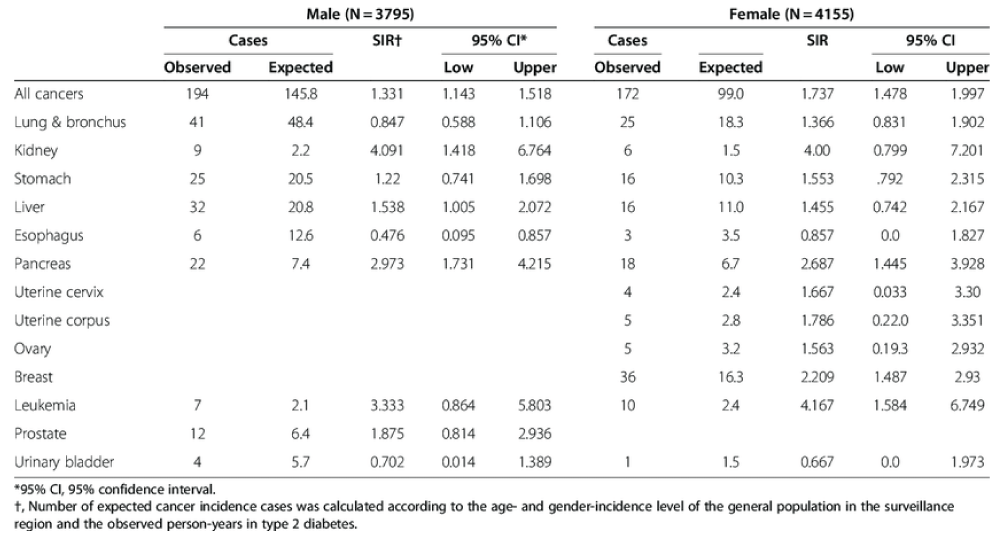
Table 2: Standardized incidence ratios (SIR’s) of cancers in patients with type 2 diabetes by gender and subtype of disease.
In the U.S and Western countries, diabetes mellitus and colorectal cancer is main reason for disease and transience as diabetes is expected to become world’s major cause of death in coming 25 years [4]. Diabetes mellitus individuals can develop oral tumor and precancerous lesions [5]. Over 400 million people had diabetes in 2015, and 17.5 million people globally had cancer. Second biggest killer in U.S is colorectal cancer. Prevalence of diabetes is expected to rise due to mounting obesity epidemic, which might leads to the expansion in other colorectal cancer cases. These discoveries demonstrate important factors in colorectal cancer involving hyperinsulinemia or insulin resistance. Though, positive interconnection of diabetes and colorectal cancer risk persisted when scientific analysis was confined to research that controlled physical activity and body mass index (summary RR = 1.34, 95%, CI = 1.20 to 1.49).
Up to 16 percent of breast cancer patients have diabetes, and breast cancer is also associated with two major risk factors for type 2 diabetes i.e. old age and obesity. A meta-analysis showed that probability of pancreatic cancer for people having diabetes is 82% greater compared to non-diabetics. Colorectal cancer (CRC) has the third highest occurrence of cancer in men and women according to the Canadian Cancer Society [6]. Countries with the highest prevalence are Europe, North America and Oceania.
It is the third common type of malignancy next to lung and breast cancer around the globe in overall population, approximately 1.24 million new cases detected in 2008 [3]. Nowadays sufficient confirmation is provided about diabetes mellitus that it is an autonomous factor for development of sarcoma [7]. The situation is uncertain, however, whether existence of diabetes mellitus is concomitant to the post-cancer prognosis among cancer sufferers. Given the cumulative incidence of diabetes wide-reaching, especially among those aged 65 and older with the maximum risk for cancer, a better comprehension of links might cause substantial consequences for healthful living. CRC is global incidence disease in world and the fourth most generally diagnosed mortality cancer, with greater rate and impermanence in males than in females in many world regions [8] (Figure 1).
Figure 1: Relationship between incidence of CRC and prevalence of DM in different parts of world.
Former studies of patients with all cause 7-10 colorectal cancer and 11-14 cancer-specific death exhibited contradictory results. An earlier systematic review of six studies available before October 2008 showed 32% upturn in diabetes-related death, plus no pooled cancer-specific mortality estimates were found [9]. As diabetes is the third largest non-cancer source of demise in people affected from CRC also intensely linked to cardiovascular disease, which is the prominent origin of non-cancer mortality in patients with colorectal carcinogenicity. Open existence and relapse must be interpreted while defining supporting part of diabetes in the diagnosis of tumor.
Enormous experiments described estimates of connotation between diabetes and cancer specific and all-causing mortality in 2008 [10]. This data provides a tremendous opportunity for accurate associative estimates to be obtained. Therefore, recent meta-syntheses objective was to find out if CRC and diabetes patients are at greater danger of all-cause and cancer-specific death in comparison to patients not having diabetes. Through results the link amongst diabetes and both disease-free survival and cancer recurrence in CRC patients was also observed. Narrative review of 21 papers testifying total mortality, comprising 216,981 applicants, presented connection of diabetes with an improved peril of all-cause loss of death among 17% of colorectal patients.
Diabetes mellitus is common prolonged disease. Majority of patients around the world have doubled over the previous three years [6]. Expected 285 million people underwent diabetes in 2010, by 2030 patients having diabetes shall upswing to 439 million, demonstrate 7.7% mature inhabitants aged 20-79 [1]. Global competition between diabetes mellitus pandemics and the increasing cancer burden has resulted in a concern to describe biological and epidemiological relationship with reference to these conditions.
Type 2 diabetes influences the standard of living. In addition to causing neural and vascular impediments, it is associated with incidence, expansion and prospects of cancer. Increasing number of therapists is considering if patients suffer from diabetes in treatment of cancer, and diabetologists in tumor-treated patients frequently cope with diabetes [7]. Countervailing hyperinsulinemia results in hormonal imbalance and metabolism also contributes in establishing microenvironments for cancer development. As a result of the insulin stimulated colorectal cancer cells evolution and insufficient management of concurrent patients, diabetes mellitus may distress endurance of carcinogenic individuals. The ramification of diabetes in cancer diagnosis was elucidated by narrative analysis [2], nevertheless since 2013, many studies have revealed comprehensive estimates of the outcome on diabetes-colorectal cancer prognosis correlation, and their effects have been reliable. Such as, in the overall survival of cancer, experiments initiated diabetes presented a substantial reduction in risk of overall existence, and no link was found in other studies. The results enabled to assess connection among them precisely. Descriptive analysis stated estimates of diabetes mellitus effect on the CRC prognosis for 5 years of survival and evaluated effects of diabetes on overall persistence of colon, colorectal and rectal cancer, cancer-specific survival (CSS), cardiovascular disease - specific survival [10] (Table 3).
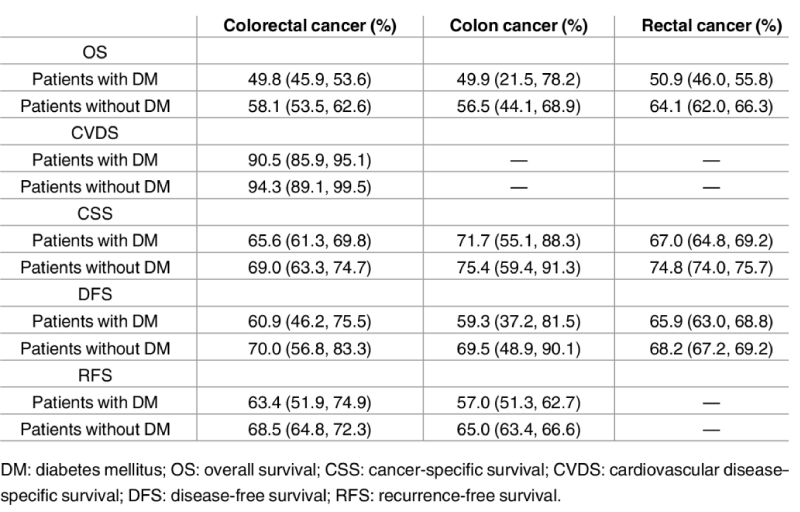
Table 3: The results indicated that compared to patients without Diabetes Mellitus, with Diabetes Mellitus will have a 5 year shorter survival rate in colorectal cancer.
Connection between Type 2 diabetes and cancer
Common risk factors: Lifestyle and diet risk factors for the improvement of diabetes and insulin resistance, like physical inactivity, obesity and ageing were concomitant with high colon cancer risk as well [7,11].
Hyperinsulinemia and Insulin treatment: A biologically possible relation of diabetes and risk of colorectal cancer was observed. At beginning stages of diabetes, it is described by elevated concentrations of insulin. There is important role of hyperinsulinemia [7] in colorectal carcinogenesis or insulin resistance factors (Figure 2). Hyperinsulinemia was suggested as fundamental connection between diabetes and colon cancer [2]. Insulin enhances cell proliferation via a small path comprising of insulin receptor or insulin-like growth factor (IGF)-I receptor’s direct activation and main pathway inhibits Insulin Growth Factor binding proteins (especially IGFBP-1 and IGFBP-2), that leads to augmented insulin growth factor-I [4]. In colorectal carcinogenesis vital part of insulin and IGF-I is held by animal models, in vitro and epidemiological studies [12]. Epidemiological studies related to circulating insulin, C-peptide or IGF-I have revealed that colorectal cancer risk in maximum exposure categories is two to three times greater than in the lowest categories of exposure. In addition, current findings stated that long-term therapy of insulin was concomitant with substantial upsurge in risk of cancer in patients diagnosed with diabetes [3]. Further processes by which diabetes is related to the colorectal cancer risk contain less passage time in diabetic patients that may leads to accelerated colonic mucosal contact to carcinogenic agents, and raised fecal bile acid concentrations in connection with high blood glucose and triglyceride concentrations [6]. In animal models, fecal bile acids were publicized to support colorectal cancer.
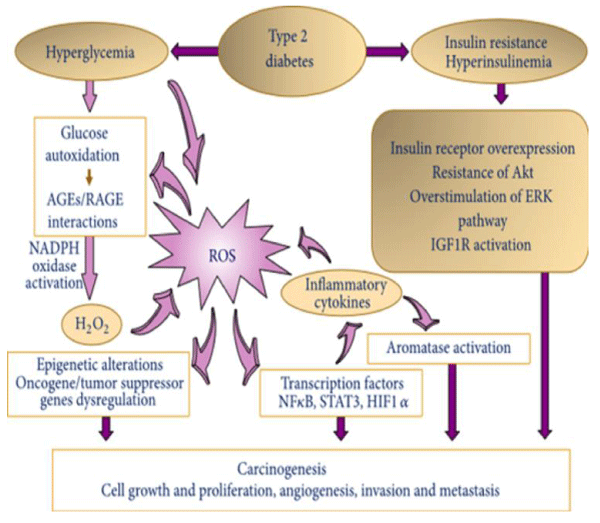
Figure 2: Pathways of oxidative stress associated with diabetes mellitus-mechanisms of carcinogenesis.
Endogenous hyperinsulinemia in diabetes mellitus might associate with a greater colorectal cancer hazard. Purpose was to decide whether or not insulin therapy could increase likelihood of colorectal cancer in population suffering from diabetes. Chronic insulin treatment considerably surges the colorectal cancer threat among people having diabetes mellitus [7]. Etiology of colorectal cancer and non-insulindependent diabetes mellitus includes westernized diet, standard of living and fatness which leads to assumption that hyperinsulinemia can stimulate colorectal cancer. Among 75,219 Norwegian male and females, we scrutinized relation concerning risk, causes of insulin resistance and hyperinsulinemia, comprising body mass index and blood glucose.
The link between the diabetes and cancer prediction is undefined at the moment. Relationship can primarily be composed on impact of cancer insulin resistance and pathogenicity on insulin-like growth factor (IGF), contributes significance part in colorectal cancer progression, and projection. IGF-1 insulin-like effects that interact with related IGF-1R, IR or hybrid receptors are very essential in maintaining average blood insulin level and diabetes mellitus abnormal condition. Insulin resistance in diabetic patients causes high secretion of insulin, which can enhance action of IGF-1, which is antiapoptic and mitogenic factor [1] by inhibiting IGF binding proteins. Conversely, in cancer cells insulin-like growth factors elevate IGF-1R also trigger intracellular signaling pathways that improve movement of cell cycle and avert programmed cell death. Zhang along with his members showed the growth of adenomatous polyps and their malignant transformation were encouraged by IGF-1 and its receptor [7]. In the colorectal cancer group IGF-1R and IR with diabetes were present over IGF-1, IGF-1R and IR expression than without diabetes mellitus [2]. Insulin dependent passage activation is acknowledged as a major stage subsidizing to numerous contrivances of cancer susceptibility to predictable and directed curative agents, resulting in greater signaling of PI3 K/Akt ultimately stops the death signals produced by chemotherapy and pacifies cells of colorectal cancer against anti-Epidermal growth factor receptor antibodies [6]. Scartozzi pronounced abundant expression of IGF-1 in patients treated by cetuximab and irinotecan with KRAS metastatic CRC wildlife was correlated with poor clinical outcomes. Their findings showed that using the IGF-1 system could empower cancerous cells to overcome anti-epidermal growth factor receptor cure due to IGF-1 augmentation of the PI3K-Akt pathway [1]. In contemporary centuries, proofs have shown IGF-1/IGF-1R polymorphisms are potential predictive markers for cetuximabic effectiveness in metastatic CRC patients with wild type KRAS [2].
Thiazolidinedione and various other peroxisome proliferator-activated receptors and ligands cause apoptosis of non - small cell lung cancer lines H841, A549, abdPC14; arrest A549 cells in the G0/G1 phase; inhibit growth and inductive DNA damage 153 genes (GADD); and make primary growth response-1 gene that cause caspase-mediated cell death.
Antidiabetic drugs
Experiments demonstrate that metformin prevents tumor and minimize risk of cancer. Latest epidemiological conclusions recommend in patients with diabetes that metformin decrease deaths from cancer [5]. Metformin therapy in diabetic patients is related with relatively less chance of colorectal cancer. Metformin is a relative of isoamylene guanidine and endorse to lower glucose as the first diabetes treatment. Earlier studies advocates metformin may be involved in suppression of tumor through the indirect instigation of Adenosine monophosphate-activated protein kinase, an important element for adenosine triphosphate and adenosine monophosphate balance of cell and helps in activation of cancer suppressor genes like LKB1. Later in vitro studies have shown that metformin hinders tumor production [13,14] and eradicate cancer stem cells [10]. Animal experiments are in agreement with such discoveries. This has been demonstrated by models of rodent that metformin can overwhelm epithelia multiplication [14,15]. Correspondingly, ability of metformin to prevent division of colon carcinoma has been shown by animal models of colon cancer [9,14]. Based on the promising research, the probable use of metformin as a new anti-inflammatory drug for the inhibition of colorectal cancer has been of interest. From this research, we combined entirely existing knowledge and appraised link of risk of metformin and colorectal cancer in type 2 diabetes patients. Consequences illustrated that therapy of metformin was related to an expected 37 percent decline in risk of colorectal cancer in people suffering from diabetes.
Biochemical pathways
Metabolic changes due to high stimulation of Wnt/beta-catenin signaling and receptor gamma suppression of response stimulated by peroxisome proliferator (PPAR gamma) can lead to the frequent link of these two diseases i.e. diabetes and colon cancer. In both diseases, PPAR gamma is down-regulated whereas it is up-regulating the canonical pathway of Wnt/beta-catenin (Figure 3A). In colon cancer, canonical Wnt system turns on which results in pyruvate dehydrogenase kinase activation and turn off pyruvate dehydrogenase complex. As a consequence, lactate dehydrogenase activation transforms a significant portion of cytosolic pyruvate into lactate. Monocarboxylate transporter-1 activation is used to extrude lactate from the cell. The process is known as Warburg’s effect. PPAR gamma antagonist brings about beta – catenin blockage, even though canonical Wnt/beta-catenin prohibition activates PPAR gamma [16] (Figure 3B). Scientific studies demonstrated connection within obesity, diabetes and cancer, specifically colon cancer [5] (Figure 4). Patients with type 2 diabetes are more likely to acquire 30%-40% colon cancer as compare to patients not having it. Diabetes risk variant leads to the threat of colorectal cancer.
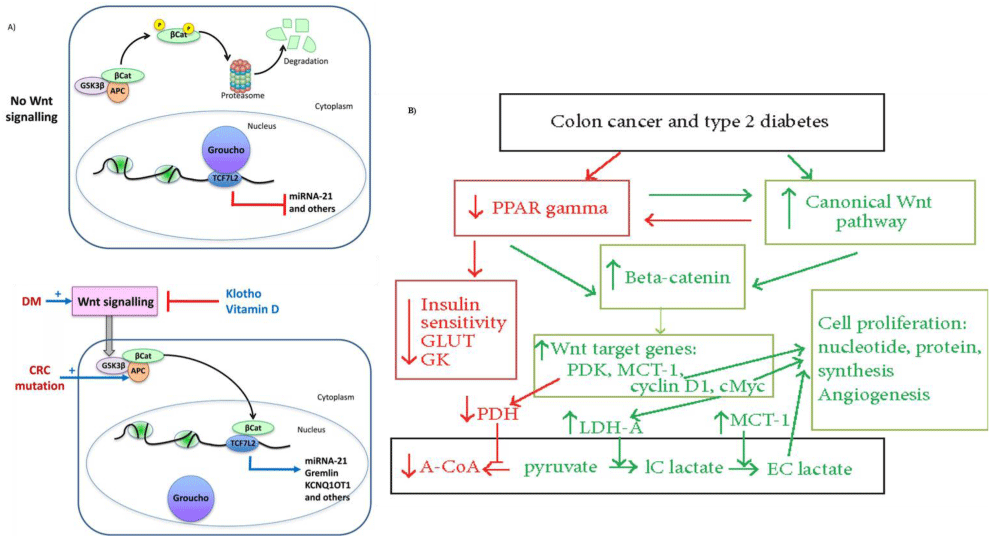
Figure 3ab: Molecular pathways linking diabetes and cancer.
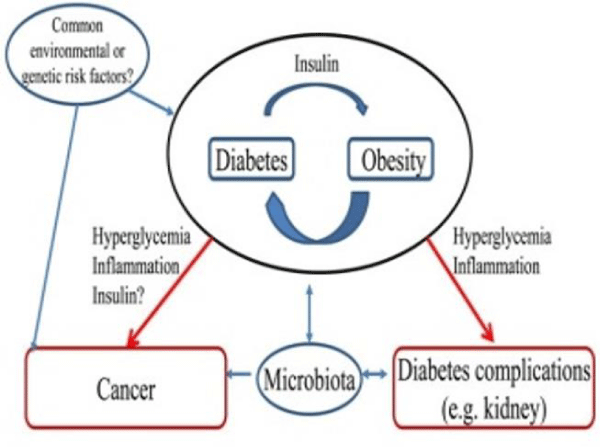
Figure 4: Hypothesis explaining association between diabetes and cancer.
The hypothesis of hyperinsulinemia in colon cancer recommends that high amount of free insulin growth factor-1 amplify cell production and better cell alteration leads to carcinogenesis. A modifying process to insulin resistance is increased insulin intensities at beginning of diabetes. Cancers, including A and IGF-1 receptors, overexpress insulin receptors. Greater amount of insulin/IGF signaling supports proliferative characteristics of both hormones. Abnormal high blood pressure and enduring tenderness can enlarge cancer growth. Activation of canonical signal initiates aerobic glycolysis or an effect of Warburg (Figure 3B). In both pathologies, Wnt activates key metabolic enzymes, like pyruvate dehydrogenase kinases (PDK). As a result aerobic glycolysis or the colon cancer effect of Warburg occurs. Reduced activity of pyruvate dehydrogenase by increased PDK alters the metabolic tractability- capability to regulate fatty acid glucose and oxidation. There is controversy for oxidation between glucose and fatty acids at the level of the pyruvate dehydrogenase complex, whose action is declined by kinase. Partial deviation in colon cancer from pyruvate to lactate leads to the synthesis of proteins needed for cell growth and propagation. The frequent association of diabetes type II with colon cancer may account in part for these major metabolic changes caused by up regulated signaling of Wnt/beta - catenin and down regulated PPAR gamma [16].
Resistance to insulin is mostly a property of diabetes connected with compensatory hyperinsulinemia. Above 250 million people worldwide have diabetes mellitus by 2010, which in 20 decades will reach to 380 million (Chowdhury, et al). Advanced studies, comprising over 2.5 million population, estimated risk of emerging colorectal in diabetics was about 30% greater than in non-diabetics [9,17-19]. The frequency of the relationship between these two diseases should be examined due to the magnitude of type 2 diabetes and cancer prevalence and the published data reports signifying the pivotal part played by diabetes among progress of colorectal malignancy [10,14]. Hence, exploring correlation between diabetes and cancer risk is evidently essential. The published data revealed inconsistent result regarding diabetes mellitus association with colorectal cancer risk. In comparison with non-diabetics, diabetics have high risk of carcinogenicity. Genome-wide association studies have recognized diabetes-related genes (e.g. TCF7L2) that can also contribute to colorectal cancer.
Epidemiological evidence recommends prevalence of cancer in association with diabetes, certain risk factors and treatment of diabetes [13]. A positive link also existed for diabetes, vulva and vaginal tumor [14]. Subsequent in vitro studies showed that metformin inhibits proliferation of carcinoma [15] and kills stem cells of cancer selectively. Metformin therapy relatively minimizes moving glucose level among individuals with too high insulin and insulin resistance. Diagnosis and treatment have made some progress in recent years, but Colorectal is major issue for the health of people even today. In order to reduce cancer mortality, there is importance of prophylaxis, evaluation and proper treatment. Factors disturbing cancer prognosis is required by policy-making system for beneficial approaches of cancer patients and improvement of disease. Eventually diabetes - specific strategies for different cancers are explored [16].
- Khaw KT, Wareham N, Bingham S, Luben R, Welch A, et al. Preliminary communication: glycated hemoglobin, diabetes, and incident colorectal cancer in men and women: a prospective analysis from the European prospective investigation into cancer-Norfolk study. Cancer Epidemiol Biomarkers Prev. 2004; 13: 915-919. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15184246
- Coughlin SS, Calle EE, Teras LR, Petrelli J, Thun MJ. Diabetes mellitus as a predictor of cancer mortality in a large cohort of US adults. Am J Epidemiol. 2004; 159: 1160-1167. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15191933
- Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, et al. Cancer statistics. CA Cancer J Clin. 2005; 55: 10-30.
- Butt A, Riaz S. Study of protein profiling of human urine in diabetic hypertensive nephropathy versus normal healthy controls. Diabetes Technol Ther. 2010; 12: 379-386. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20388048
- Zhi-Jie Z, Haidong K, Yiqing S, Wei C, Genming Z, et al. Reduced risk of colorectal cancer with metformin therapy in patients with type 2 diabetes: a meta-analysis. Diabetes care. 2011; 34: 2323-2328. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/21949223
- Schulze MB, Hu FB. Primary prevention of diabetes: what can be done and how much can be prevented? Annu Rev Public Health. 2005; 26: 445-467. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15760297
- Larsson SC, Giovannucci E, Wolk A. Diabetes and colorectal cancer incidence in the cohort of Swedish men. Diabetes Care. 2005; 28: 1805-1807. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15983343
- Gong YW, Benjuan YL, Weijuan. Type 2 diabetes mellitus and risk of oral cancer and precancerous lesions: A meta-analysis of observational studies. Oral Oncol. 2015. 51. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25650271
- Mills KT, Bellows CF, Hoffman AE, Kelly TN, Gagliardi G. Diabetes Mellitus and Colorectal Cancer Prognosis: A Meta-analysis. Dis Colon Rectum. 2013; 56: 1304-1319. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/24105007
- Zhu B, Wu X, Wu B, Pei D, Zhang L, et al. The relationship between diabetes and colorectal cancer prognosis: a meta-analysis based on the cohort studies. PloS one. 2017; 12. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28423026
- Yasemin S. Diabetes May Increase Risk for Cancer, Especially for Women. 2018.
- Aura DHM, Sergio PA, Fernando LL, Manuel DG, María AGM, et al. Type 2 Diabetes in Neuroendocrine Tumors: Are Biguanides and Statins Part of the Solution? J Clin Endocrinol Metab. 2018; 1: 57-73. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30265346
- Guraya SY. Association of type 2 diabetes mellitus and the risk of colorectal cancer: A meta-analysis and systematic review. World J Gastroenterol. 2015; 21: 6026. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/26019469
- Kathleen K. The Cancer-Diabetes Connection. 2018.
- Barbara AMara. Diabetes mellitus and cancer risk: A multisite case-control study. J Chronic Dis. 1985; 435-441. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3998058
- Lecarpentier Y, Claes V, Vallée A, Hébert J. Interactions between PPAR Gamma and the Canonical Wnt/Beta-Catenin Pathway in Type 2 Diabetes and Colon Cancer. PPAR research. 2017. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28298922
- Larsson SC, Orsini N, Wolk A. Diabetes mellitus and risk of colorectal cancer: a meta-analysis. J Natl Cancer Inst. 2005; 97: 1679-1687-1987. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16288121
- Vernieri C, Galli F, Laura F, Sara L. Impact of Metformin Use and Diabetic Status during Adjuvant Fluoropyrimidine‐Oxaliplatin Chemotherapy on the Outcome of Patients with Resected Colon Cancer: A TOSCA Study Subanalysis. The oncologist. 2019; 2018: 0442. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30606884
- Fransgaard T, Thygesen LC, Gögenur I. Metformin increases overall survival in patients with diabetes undergoing surgery for colorectal cancer. Ann Surg Oncol. 2016; 23: 1569-1575. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/26714936